

Blood Transfusion in Cats & Dogs
A blood transfusion is a medical procedure used in dogs to treat symptoms of anemia caused by disease, surgery, toxicity, or trauma. The goal of blood transfusion is to treat symptoms caused by anemia by replacing red blood cells so that proper oxygenation of organs can occur. Blood transfusions are most often used in acute situations such as acute hemolysis or blood loss, but can also be used for chronic conditions such as immune mediated hemolytic anemia. Not all patients with anemia require a blood transfusion. Blood transfusions are administered by a veterinarian in the veterinary clinic.
Before receiving a blood transfusion, your dog will be cross-matched with the donor blood to determine compatibility. This is especially important for those patients who received a blood transfusion more than three days prior and need another transfusion. Your dog may also have coagulation testing done to determine the need for a plasma transfer. Blood transfusion is typically done to stabilize a patient with symptoms of anemia. It may need to be repeated until the primary cause of anemia is managed. There is usually no need for anesthesia for a blood transfusion to be performed.
After preliminary testing is done to ensure your dog is a match with the donor blood, an IV will be placed for the blood transfusion. If a catheter is already in place, a separate line will be added to ensure that only the blood product is traveling in the line. The transfusion could last from one to four hours. One hour for patients who are unstable and have life threatening signs of anemia and four hours for patients with mild to moderate symptoms of anemia, allowing for close observation in case of an adverse reaction.
Once the transfusion is done, your dog will be monitored for several hours to ensure that they are stable. Your veterinarian will check your dog’s vital signs and perform blood tests to monitor the resolution of the anemia. Your dog will also be monitored for signs of an adverse reaction such as vomiting, increased respiratory effort, edema or hives.
Since the early 80s the use of blood products in treating critically ill animals and supporting animals undergoing surgical and other procedures has tremendously increased. However, it should be noted that blood products are prepared from donor animals and represent a very limited resource not available in all situations, and as they are biologicals they bear the inherent risks to transmit infectious agents and cause other adverse transfusion reactions. Furthermore, the need for blood typing and crossmatching of patients and donors has now been recognized in order to assure safe and more efficacious transfusions in dogs and cats. Veterinary clinicians play a key role in providing safe and effective transfusion therapy and therefore they need to be aware of the transfusion principles.
Here some key points:
Transfusion therapy refers to the safe and effective replacement of blood or one of its components offering support for many critically ill anemic and bleeding patients.
The indications for transfusions need to be clearly determined, and ideally only the deficient blood component is replaced at the appropriate dose.
While red blood cells and plasma clotting factors are crucial, the indications and efficacy of transfusing platelets, leukocyte, as well as other plasma proteins are limited.
Blood products represent a limited resource; hence they should only be given when indicated, at the minimal dose required and after carefully considering all alternatives.
All blood donors need to be typed for DEA 1.1 and the feline AB blood groups, resp., and regularly screened for their health including testing for infectious diseases.
All recipients should be typed for DEA 1.1 and feline AB and any previously transfused (>4 days) animals should also be crossmatched prior to the next red cell transfusion.
While acute hemolytic transfusion reactions are feared most, they can be avoided by prior compatibility testing; other adverse transfusion reactions may not be predicted.
The efficacy of survival of transfused blood cells and plasma proteins should be monitored during and post-transfusion with the appropriate clinical and laboratory parameters.
Indications for Transfusion Therapy
Transfusions are indicated for anemia, coagulopathy, and rarely for other conditions such as thrombocytopenia/-pathia, and hypoproteinemia. However, the decision to transfuse is based upon the overall clinical assessment of a patient’s history and clinical signs, routine laboratory tests, underlying cause, and hence sound clinical judgment. And because of the inherent risks, transfusions should never be given without a clear indication and exhausting other alternatives.
The most common indication for a transfusion in dogs and cats are anemias and depending on the type, degree and course of the anemia a transfusion with blood products, such as stored packed red cells, fresh or stored whole blood, may be warranted. Animals with rapidly progressive anemia need to be transfused much earlier, when the PCV is still around or above 20%, while patients with chronic anemias may do well at lower hematocrits as long as they are not stressed. It should be noted that animals with peracute blood loss will not show a drop in PCV for hours until fluid shifts have occurred. Hence, other parameters, such as evaluation of mucous membranes and capillary refill time, are needed to assess the hypovolemia and need for blood transfusions. Fluid therapy may be all that is needed to restore vital organ perfusion in acute blood loss anemias, while packed red blood cells (pRBCs) are considered, when there is evidence of tissue hypoxia. In other words the associated lowering of the PCV is no contraindication for fluid therapy to restore normovolemia. Furthermore, if an animal needs to undergo anesthesia and surgery, generally the PCV should be at least 15-20% to assure proper oxygenation during the procedure. Red cell transfusions have proven life-saving in cases of immune-mediated hemolytic anemia and there is no evidence that transfused red cells would be more rapidly destroyed than the patient’s erythrocytes or that they “add to the fire”, although some clinicians have questioned their value.
Fresh frozen plasma (FFP) is most commonly used to treat coagulopathies causing serious bleeding in veterinary practice as it contains all coagulation factors. Hemorrhage caused by acquired coagulopathies such as liver disease and anticoagulant rodenticide intoxication, just like bleeding due to any of the many hereditary coagulopathies are certainly common indications. Sudden bleeding due to therapeutically used heparin or warfarin to counter thrombosis can also successfully be corrected with FFP. The use of FFP (to replace deficient coagulation factors as well as antithrombin) with or without heparin in the management of disseminated intravascular coagulation remains controversial; there are no studies documenting any definitive beneficial effects. Similarly, evidence for FFP to help in acute pancreatitis (to replace alpha-macroglobulins) or in parvovirosis (to provide anti-parvo and other immunoglobulins and stop gastrointestinal hemorrhage) is lacking. FFP is also commonly used to correct hypoproteinemias, but its effect on the oncotic pressure in cases of protein-losing nephropathies and enteropathies is minimal for the FFP doses that are typically administered and practically available. Note lyophilized canine albumin has just become commercially available.
Other blood products are less commonly used in dogs and are not generally available for cats. Cryoprecipitate is rich in fibrinogen, fibronectin, and the von Willebrand factor VIII complex and is the preferred treatment for bleeding dogs with these plasma protein deficiencies. If available, cryo-poor plasma may be administered to hypoproteinemic dogs, where synthetic plasma expanders are insufficiently effective or in case of anticoagulant rodenticide poisoning. Because platelets are relatively short-lived (one week) and cannot readily be stored for any length of time (<24 hours at room temperature), platelet rich plasma and concentrate are rarely transfused. Hemorrhage caused by thrombocytopenia in anemic dogs could be managed with fresh whole blood, but generally only requires the use of pRBCs to correct the anemia. Rarely platelet-rich plasma and platelet concentrates are required to control life-threatening bleeding. Furthermore, in dogs with immune-mediated thrombocytopenia transfused platelets have a very short half-life of hours, and albeit they may be helpful to control life-threatening hemorrhage such transfusions will not result in any appreciable platelet rise. Because of the very short normal half-life of granulocytes (hours) leukocyte transfusions are not generally practiced in human and veterinary medicine.
Canine and Feline Blood Types
To assure efficacious and safe transfusions, blood donor and recipient should be blood typed and if previously transfused also crossmatched. Blood types are genetic markers on erythrocyte surfaces that are antigenic and species specific. A set of blood types of two or more alleles makes up a blood group system. Because administration of a small amount (<1ml) of incompatible blood can result in life-threatening reactions, this practice to assess blood type compatibilities is unacceptable???. Blood typing is clinically important to assure blood compatibility and therefore is recommended for any animal in need of a transfusion or considered to become a blood donor. Unless blood typing is regularly performed in practice, it is best to send blood for typing to a reference laboratory. There are typing cards (DMS) and cartridges (Alvedia DME) for in-clinic use as well as gel column assays for reference laboratories. Caution should be exercised whenever the patient’s blood is autoagglutinating or has a very low hematocrit (<10%).
In dogs, the clinically most important blood type is DEA 1.1: DEA 1.1 (A1) elicits a strong alloantibody response after sensitization of a DEA 1.1 negative dog by a transfusion; thus can be responsible for a transfusion reaction in a DEA 1.1 negative dog previously transfused with DEA 1.1 positive blood. Transfusion reactions against other blood types have rarely been described. They include reactions against the DEA 4, Dal and another common red cell antigen, and other clinically important blood types may be found in the future. There are no clinically significant alloantibodies present prior to sensitization of a dog with a transfusion (no sensitization by pregnancy).
The major feline blood group system thus far generally recognized is known as the feline AB blood group system and contains 3 alleles: type A, type B, and the extremely rare type AB. Most domestic shorthair cats have type A blood, but the proportion of type B cats can be substantial in certain areas. The frequency of A and B blood types also varies greatly between different breeds, but likely not much geographically in purebred cats. Most blood donors have type A blood, but some places also keep cats with the rare type B and type AB as donors. All blood donors must be typed. Naturally-occurring alloantibodies have been well documented in type A and type B cats and require that blood typing be performed prior to both blood transfusion and breeding to assure appropriate blood compatibility. All type B cats have very strong naturally-occurring anti-A alloantibodies. They are responsible for serious transfusion reactions. Furthermore additional blood group systems are being identified such as the Mik red cell antigen in Domestic shorthair cats; Mik-negative cats may produce naturally occurring alloantibodies.
Whereas blood typing tests reveal the blood group antigens on the red blood cell surface, blood crossmatching tests assess the serologic compatibility or incompatibility between donor and recipient. Thus, the crossmatch test checks for the presence or absence of naturally occurring and induced alloantibodies in serum (or plasma) without determining the blood type. These antibodies may be hemolysins and/or hemagglutinins and can be directed against known blood groups or other red cell surface antigens. Beside a standardized tube crossmatching procedure there is a laboratory gel column (DiaMed) as well as tube gel test (DMS) available. The major crossmatch tests for alloantibodies in the recipient’s plasma against donor cells, whereas the minor crossmatch test looks for alloantibodies in the donor’s plasma against the recipient’s red blood cells. A minor crossmatch incompatibility should not occur in dogs if canine donors have not been previously transfused and is of lesser concern because donor’s plasma volume is small, particularly in packed red cell products, and will be markedly diluted in the patient. In contrast, the major and minor crossmatch can show incompatibility prior to any transfusion due to the presence of naturally occurring alloantibodies in cats, not only for the AB but also the Mik and possibly other blood group systems. The initial blood crossmatch between two dogs that have never received a transfusion before should be compatible, because dogs do not have naturally occurring alloantibodies. Therefore, one might omit a crossmatch before the first transfusion in clinical practice. Obviously, a blood donor should never have received a blood transfusion to avoid sensitization. In cats, mixing a drop of donor/recipient blood with donor/recipient plasma will detect A-B incompatibilities if typing is not available.
Blood Donors Sources and Collection
Many larger veterinary hospitals have permanent canine and/or feline blood donors to cover their transfusion requirements or in case fresh whole blood or platelet-rich plasma (concentrate) is needed. Several larger voluntary blood donor programs have emerged with client or staff owned dogs. More than a dozen commercial canine blood banks have been established in the United States and deliver overnight blood products; however, there is generally a shortage. Some are also providing feline products. Autologous (self) transfusion refers to the donation of blood by a patient four weeks to a few days prior to surgery when major surgical blood loss is anticipated. Blood can also be collected immediately prior to surgery. The patient will be hemodiluted with crystalloid and colloid solution and receives the blood when excessive bleeding occurs or after surgery. Autotransfusion is another autologous transfusion technique in which shed blood salvaged intra-operatively or following trauma can be reinfused after careful filtering. However, do not reinfuse blood from long-standing (<4 hours; shouldn’t it be >4 hours???), contaminated, or malignant hemorrhagic effusions.
Blood donors should be young adult, lean, and good tempered animals, and weigh at least 23 kg for dogs (to donate 450ml) and 4 kg for cats (40ml); have no history of prior transfusion; have been regularly vaccinated and are healthy as determined by history, physical examination, and laboratory tests (complete blood cell count, chemistry screen, and fecal parasite examination every 6-12 months), as well as free from infectious diseases (testing depends on species/breed and geographic area but may include serology, antigen assays and PCR assays). Donors should receive a well-balanced, high performance diet, and may be supplemented twice weekly with ferrous sulfate (Feosal, 10 mg/kg), if bled every 4 weeks. Packed cell volume (PCV) and hemoglobin (Hb) should be >40% and >13 g/dl in canine donors and >30% and >10 g/dl in cats.
Canine donors are generally not sedated, while cats are regularly sedated with a combination of ketamine (10 mg), diazepam (0.5 mg), and atropine (0.04 mg) by intravenous injection. Some sedatives, such as acepromazine, interfere with platelet function and induce hypotension, hence they should not be used. Blood is collected aseptically by gravity or blood bank vacuum pump from the jugular vein over a 5 to 10 minute period. Plastic bags containing citrate-phosphate-dextrose-adenine (CPD-A1) with or without satellite bags for blood component separation are optimal. These commercial blood bags represent a closed collection system in which the blood does not come into contact with the environment at any time during collection or separation into blood components, thus minimizing the risk for bacterial contamination and allowing storage of the blood products. A large plastic syringe containing 1 ml CPD-A1 or 3.8% citrate per 9 ml blood and connected to a 19 gauge butterfly needle is commonly used for cats. This represents an open collection system in which connections allow exposure of blood to the environment; because of the potential risk for bacterial contamination, blood collected via an open system should not be stored for more than 48 hours. Vacuum glass bottles containing acid-citrate-dextrose (ACD) allow rapid collection, but are not recommended because blood components are readily damaged and cannot be separated and stored for long. The maximal blood volume to be donated is 20 ml blood/kg or one regular blood bag unit of 450 ± 45 ml per > 25 kg dog and 10 ml blood/kg or 50 ml blood (one typical feline unit) per > 5 kg cat.
Blood components are prepared from a single donation of blood by simple physical separation methods such as centrifugation generally within 8 hours from collection; thereby, fresh whole blood can be separated into packed red cells, platelet-rich plasma or concentrate, fresh frozen plasma, and cryoprecipitate and cryo-poor plasma. Blood component preparation is best accomplished by using plastic blood bags with satellite transfer containers in order to assure sterility. Fluctuations in storage temperature significantly alter the length of storage; thus, temperature controlled and alarmed blood bank refrigerators and freezers are ideal, but others are acceptable as long as the temperature is monitored and the refrigerator/freezer is not too frequently opened. Blood components that have been warmed to room or body temperature should not be recooled and cannot be stored again. Similarly, partially used or opened blood bags should be used within 24 hours because of the risk of contamination.
Administration of Blood Products
For routine transfusion in the treatment of anemia, it is not necessary to warm blood after removal from the refrigerator. Warming may in fact accelerate the deterioration of stored red blood cells and permit rapid growth of contaminating microorganisms. However, there are specific clinical situations such as transfusion of neonates or resuscitation of trauma patients necessitating rapid, massive transfusions, in which warming of blood is indicated to prevent complications associated with hypothermia (e.g., cardiac arrhythmias and coagulopathies). A temperature-controlled waterbath (37°C) is ideal to warm blood products. A warm water bowl in which the water is periodically changed may be used to warm blood products. Care should be taken to maintain absolute sterility and to not overheat the blood products. Blood components that have been prewarmed cannot be refrozen/refrigerated.
Blood bags are connected to blood infusion sets that have an in-line microfilter. A long (85 cm) blood infusion set with a dripping chamber and a short infusion set for small dogs and cats to connect with syringes are available. Use a latex-free infusion set for platelet administration to avoid aggregation. Microfilters with 170 µm pores are commonly used to remove clots and larger red cell and platelet aggregates. Finer filters with 40 µm pores will remove most platelets and microaggregates and clog after 50 ml. Leukocyte reduction filters (expensive) may be used to decrease febrile adverse reactions to WBC components. Sterility has to be maintained when connecting blood component bag to infusion set and tubing to catheter.
Blood components are best administered intravenously. Ideally, an indwelling catheter (16-22 gauge depending on size of animal) is placed into the jugular vein, but the cephalic or saphenous vein on extremities or intraosseous catheters may also be used. Avoid concurrent feeding and administration of drugs or fluids other than physiologic saline through the same catheter in order to prevent lysis of erythrocytes and blood coagulation.
Rate of transfusion depends on the hydration status, degree of anemia, and general health condition of an animal. Initial rate is slow, starting with 1-3 ml over the first 5 minutes to observe for any transfusion reactions, even with blood typed and/or crossmatched transfusions. In animals with cardiac failure, do not exceed 4 ml/kg/hr. Transfusion of a single bag should be completed within 4 hours to prevent functional loss or bacterial growth. Volume of blood component to be administered depends on the type of deficiency and size of the animal. In anemia: Volume (ml) of whole blood = 2 x PCV rise desired (%) x body weight (kg) or in other words, administration of 2 ml whole blood/kg body weight raises the PCV by 1%. If packed red cells are used without prior resuspension in a red cell preservative, half the volume has to be administered, since packed red cells have a PCV of 70-80%. In the absence of bleeding and hemolysis, at least 70% of transfused erythrocytes survive 24 hours (required blood bank standard) and transfused erythrocytes may be thereafter expected to have a normal life-span (approximately 70 days in cats, 110 days in dogs). Monitor response to transfusion by obtaining PCV/TP readings prior to, immediately, and 6 and 24 hours post-transfusion, and consider continued blood loss and/or hemolysis.
In thrombocytopenia or thrombocytopathia, one unit of PC, PRP or FWB will increase the platelet count by 10,000/µL in a recipient weighing 30 kg. In animals with serious or life-threatening bleeding, the platelet count should be increased to >40,000/µL. Platelet counts are monitored prior to, 1 hour and 24 hours after the platelet transfusion.
In coagulopathies and von Willebrand’s disease, FFP at 6-10 ml/kg is an initial dose to stop bleeding or avoid excessive bleeding during surgery. In some cases, larger volumes may be needed to control bleeding. Depending on the coagulopathy, repeated administration of FFP may be required. Because of the short half-life of factors VII and VIII and von Willebrand factor, deficient animals need to be treated twice to four times daily. Other coagulopathies may be treated daily. Cryoprecipitate at a dose of 1 CRYO unit/10 kg or 1-2 ml/kg body weight twice daily is ideal to treat hemophilia A and von Willebrand’s disease. Plasma support should be provided for an additional 1-3 days after the bleeding has been controlled to allow for healing and prevent rebleeding.
Adverse Transfusion Reactions
While transfusion of blood and its components is usually a safe and temporarily effective form of therapy, there is always a risk for potential hazards. Adverse reactions usually occur during or shortly after the transfusion and can be due to any component of whole blood. Most transfusion reactions can be avoided by carefully selecting only healthy donors, using appropriate collection, storage, and administration techniques, performing blood typing and crossmatching, and administering only needed blood components. The most common clinical sign of a transfusion reaction is fever, followed by vomiting and hemolysis. Hemolytic transfusion reactions can be fatal and are, therefore, most important, while fever and vomiting are usually self-limiting. Adverse effects of transfusions can be divided into non-immunologic (pyrogen-mediated fever, transmission of infectious agents, vomiting, mechanical hemolysis, congestive heart failure, hypothermia, citrate toxicity, pulmonary complications) and immunologic reactions (acute and delayed hemolytic transfusion reactions, urticaria to anaphylaxis, graft versus host disease). Note that some clinical signs may be caused by both mechanisms. In surveys of blood product usage, transfusion reactions were observed in 2-13% of recipients, but none of them were definitely associated with blood group mismatches and hence could have been caused by other blood components or blood collection, processing and storage as well as host factors.
In private practice, blood donations often come from animals living at the hospital or from the pets of employees or clients. Both dogs and cats can donate blood to help save the lives of critically ill animals, but many considerations need to be taken into account when choosing the most qualified dogs and cats to be used as donors.
Requirements for Blood Donors
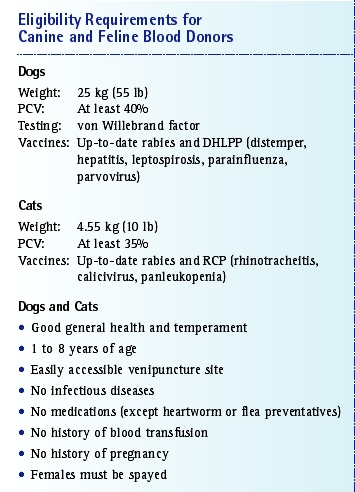
To be eligible for blood donation, dogs and cats must have good general health and temperament and be between 1 to 8 years of age. A minimum weight is required: dogs should weigh at least 25 kg (55 lb) and cats should weigh at least 4.55 kg (10 lb). These weights allow 450 ml of blood to be collected from a dog and 60 ml from a cat without any harm to the donor. The donor’s packed cell volume (PCV) also must be within certain limits. In dogs, the PCV should be at least 40% (normal range: 37% to 55%); in cats, it should be at least 35% (normal range: 30% to 45%).The PCV has to be checked before each donation to make sure the requirements are met. Dogs that are going to be regular donors should also be tested for von Willebrand factor to make sure their platelet function is normal.
All blood donors should have up-to-date vaccinations, including rabies and DHLPP (distemper, hepatitis, leptospirosis, parainfluenza, parvovirus) for dogs and rabies and RCP (rhinotracheitis, calicivirus, panleukopenia) for cats.2-4 However, modified-live virus vaccine may affect platelet and endothelial function for up to 10 days postvaccination; therefore, blood should not be donated until 11 days after the dog or cat is vaccinated.
Donors should not have an infectious disease that might be transmitted through a blood transfusion: Dogs must be free of bacterial infections (e.g., ehrlichiosis, borreliosis), dirofilariasis, trypanosomiasis, babesiosis2,3; cats must be free of bacterial infections (e.g., hemobartonellosis), FeLV, and FIV. Donors should not be receiving any medication other than heartworm or flea preventatives and should never have received a blood transfusion.2,5 Female dogs and cats should be spayed and have no history of pregnancy. Only indoor cats should be used as blood donors. In addition, all donors should have an accessible venipuncture site to allow for easy blood collection.
Although dogs and cats that meet all the eligibility requirements can donate blood every 4 to 5 weeks, most donor programs have multiple donors so that each donor usually donates about four times per year but can be used more often if necessary. Having a large pool of eligible blood donors is desirable because it reduces the likelihood that any one donor will be used too often. Repeat donors should be tested for parasites and have a complete blood cell count and chemistry profile performed yearly; dogs should be tested annually for heartworm disease.
Blood Types
Blood types are genetic markers on red blood cells (RBCs) that are antigenic and vary between species.2,3,6
Canine Blood Groups
At least 12 canine blood groups have been identified, and their names have changed many times since they were discovered. The canine blood groups used to be named alphabetically (e.g., A1, A2, B, C) but are now designated by the acronym DEA (dog erythrocyte antigen) and a number (e.g., DEA 1, DEA 2, DEA 3). DEA 1 has two alleles of interest: 1.1 and 1.2. DEA 1.1-positive is the most common canine blood type, and dogs with this blood type are considered universal recipients. Dogs with blood that is negative for DEA 1.1 and DEA 1.2 are in many cases considered “universal” donors. DEA 1.1-positive is considered the most antigenic blood type in dogs, and the antibodies may result in acute hemolysis if this blood type is transfused incorrectly (e.g., if DEA 1.1-positive blood is given to a dog that has previously been sensitized to this blood type).DEA 1.2-positive interactions also have been documented, although they are less severe than DEA 1.1-positive interactions. Significant naturally occurring alloantibodies are not seen in dogs; therefore, antigen-antibody reactions are less likely on initial transfusion.2,6 Dogs with immune-mediated diseases (e.g., immune-mediated hemolytic anemia) can have a reaction on initial transfusion because their body is already attacking its own RBCs. It is expected that the transfused RBCs will be lysed at the same rate as the patient’s RBCs until immune suppression occurs.In these patients, multiple transfusions may be needed. After the first transfusion, most dogs become sensitized to the type of blood they received and must be crossmatched before receiving any more blood.2,6 Sensitization may also occur during pregnancy. If the dog has never received a transfusion or been pregnant, the results of crossmatching would show compatibility regardless of the donor’s blood type.
Feline Blood Groups
In cats, three blood groups have been identified: A, B, and AB. Although type A is the most common blood type in cats overall, type B is common in certain purebreds (e.g., Devon rex, Abyssinian, British shorthair). Type AB is rare and is not the same as human blood type AB. Because cats have naturally occurring alloantibodies against the blood type antigen they lack, there is no universal feline blood donor. For example, type B cats have high anti-A alloantibodies and type A cats have weak anti-B alloantibodies. Therefore, if a cat is transfused with blood that matches its own blood type, the RBCs will have a half-life of 29 to 39 days. However, if a type A cat is transfused with type B blood, a mild reaction may occur and the RBCs will have a half-life of approximately 2 days. If a type B cat is transfused with type A blood, the RBCs will be rapidly destroyed (within a few minutes to hours) and severe clinical signs, or even death, will likely result. The bottom line, then, is that type A cats should receive only type A blood and type B cats should receive only type B blood. However, type AB cats can receive either type A or type B blood with minimal to no clinical reactions.
Another serious outcome of blood group incompatibility occurs in type A kittens bred from a type B queen and a type A tomcat. This condition, called neonatal isoerythrolysis, is caused by the destruction of RBCs in the kitten by naturally occurring anti-A antibodies in the mother’s colostrum.5,8 Neonatal isoerythrolysis can be prevented by crossmatching or blood-typing cats before breeding them.
Blood-Typing
Blood-typing is a method of identifying the antigens on RBC surfaces. Blood types may be determined by sending samples to a laboratory or by using commercially available blood-typing cards. These cards are available for both feline and canine blood-typing and can detect DEA 1.1 and feline types A, B, and AB. Blood-typing cards are relatively simple to use, but the results may not always be easy to interpret. Whenever the blood type cannot be determined with certainty in the clinic, samples should be sent to a diagnostic facility for confirmation. In samples of canine blood that is potentially DEA 1.1-negative, the laboratory can also type the blood for DEA 1.2 to confirm that the RBCs are negative for both DEA 1 alleles, which would mean the dog is a “universal” donor.
Blood-typing animals before they participate in a blood donor program is crucial to ensure that the transfusion recipient is given the right blood type, especially if there is a chance the recipient has been sensitized to the blood received in a previous transfusion.2,10 Because cats have antigens against the blood types they lack, mismatched blood can be fatal. Because dogs do not have naturally occurring antigens against the blood types they lack, it is more important to crossmatch than blood-type a canine recipient before transfusion.2,5
Crossmatching
The crossmatch is a laboratory test that predicts a transfusion recipient’s response to a donor’s RBCs and plasma by detecting any serum (plasma) incompatibility between the donor and the recipient.Crossmatching is a two-part procedure. The major part of the test assesses whether there are antibodies in the recipient’s plasma that might cause a hemolytic reaction to the donor’s RBCs. The minor part detects antibodies in the donor’s plasma that might react to the recipient’s RBCs.In both parts of the crossmatch, incompatibility is signaled by the agglutination of RBCs.
Because healthy dogs do not have naturally occurring alloantibodies, a crossmatch does not have to be performed on a dog receiving a transfusion for the first time unless the recipient has been diagnosed with an immune-mediated disease. Because it takes about 3 days for a dog to become sensitized to transfused blood, crossmatching also need not be done on a dog transfused within the previous 72 hours. If a dog received a transfusion more than 72 hours previously or has a history of pregnancy, crossmatching should be done in case sensitization has occurred. In emergency situations in which there is no time for crossmatching or blood-typing, the dog should be given type DEA 1.1-negative blood.
Crossmatching should be performed on cats with unknown blood types if a blood-typing card is not available. Because of the naturally occurring alloantibodies in cats, feline blood types can be predicted based on the blood crossmatch results.
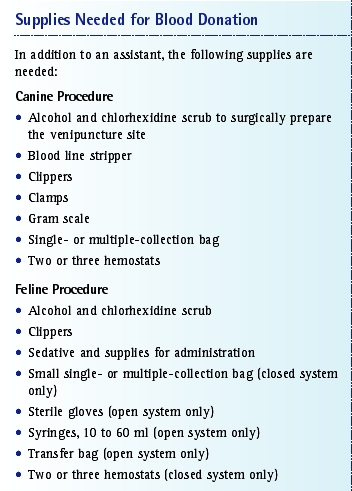
Collection Process
Blood is collected using either a closed or an open system. In both systems, blood is collected using strict aseptic technique and sterile equipment to help reduce the risk of bacterial contamination. Blood collection is performed similarly in cats and dogs; in cats, an open system is used more frequently than a closed system. Both single- and multiple-collection bags are available. Because cats can donate a maximum of only 60 ml of blood, the multiple-collection bags used for dogs are too big for cats. There are, however, smaller multiple-collection bags available for feline donation as well as small single-collection bags that are more appropriate for the amount of blood collected from cats. Although the relatively small amount of blood that can be collected from cats also makes component preparation more difficult, this goal can be achieved if the transfusion recipient would benefit more from a blood component (e.g., packed red blood cells [pRBCs], plasma) than from whole blood.
The jugular veins are the best sites for canine or feline blood collection because they are easily accessible, are larger than the other veins, and carry a large volume of blood, which helps minimize RBC trauma during collection. Ideally, blood should be collected using a single, uninterrupted venipuncture to avoid cell damage and excessive activation of coagulation factors.
For blood collection, the donor is placed in lateral recumbency. The side of the animal used for collection depends on the preference of the person drawing the blood, but it is important to alternate jugular veins with each donation. Sedation is optional for canine donors but required for cats because they are less likely to be still during the period required for blood collection.
After the blood collection process is complete, donors should be offered a small meal and plenty of water along with rest. The donor’s body immediately starts to replace the blood that was given for donation, and the donor’s blood is completely replaced within 21 days.
Closed System
A closed system allows for the collection, processing, and storage of blood and blood components without exposing them to the environment; therefore, the risk of bacterial contamination is minimized. This system is the one most often used in canine blood collection but is sometimes used in feline blood collection as well.
The steps for collecting blood using a closed system are listed in the box above. For this procedure, single-collection bags are available that contain an anticoagulant solution plus integral tubing with a 16-gauge needle already attached. Although this system is not recommended for component preparation, it can be used for this purpose if absolutely necessary. After collection, the whole blood is spun down at 5,000 xg for 15 minutes with a refrigerated centrifuge and the plasma is transferred to a transfer pack. pRBCs are left in the original collection bag. Also available are multiple-collection bags containing an anticoagulant solution and two or three satellite bags for component preparation. The multiple-bag collection system is primarily used over single-collection bags to make component preparation easier.
Open System
In an open system of collection (e.g., drawing blood with a syringe), blood and blood components are exposed to the environment, a disadvantage compared with the closed system. This system is mostly used in feline blood collection but may be used in canine collection if necessary. For example, if only a small amount of blood is needed (e.g., for transfusion in a puppy), a syringe may be used to obtain the exact amount from the donor.
The open system most commonly used in feline blood collection is the syringe method.For this technique, a 19- to 21-gauge butterfly catheter is inserted into the jugular vein. When the catheter is filled with blood, a syringe containing the correct amount of anticoagulant is attached. Although syringes used for this purpose can range from 10 to 60 ml, the 60-ml syringe is used most often because it reduces the risk of contamination, which is greater when two smaller syringes are used consecutively. The plunger on the syringe is gently pulled back, and as the syringe fills with blood, it is inverted to allow the anticoagulant and the blood to mix, which prevents clot formation. After the blood is collected, it is transferred to a blood collection bag or transfer pack or is transfused into the recipient directly from the syringe. Because this method is the one most commonly used in cats, feline transfusion patients usually receive fresh whole blood (FWB) instead of stored blood.
Blood Products
Although whole blood is most commonly used in feline transfusion, canine recipients are usually given blood components. Whole blood can be separated into pRBCs, fresh-frozen plasma (FFP), frozen plasma for long-term storage, platelet-rich plasma (PRP), platelet concentrate, and cryoprecipitate. Blood component therapy has several advantages over whole blood:
- It allows for more specific replacement of an animal’s deficits.
- It decreases the risk of transfusion reactions.
- It allows for more efficient use of the blood donor.
All blood products should be stored separately, away from all other items. Storage is especially crucial for blood products that must be kept frozen. For these components, an automatic defrosting freezer is best. The freezer should be dedicated to plasma storage only, as continual opening and closing of the freezer door will affect factor activities. The temperature should be kept at a maximum of 4°F (-20°C) with minimal fluctuation, and temperature checks should be performed daily.
Whole Blood
FWB is blood that is less than 8 hours old, has not been refrigerated, and is composed of RBCs, leukocytes, platelets, coagulation factors, and plasma proteins. FWB is indicated for acute bleeds, anemia with coagulation deficiency, and disseminated intravascular coagulation and can also be used in massive transfusion.To achieve the full benefits of all components, FWB should be administered immediately after collection.
Stored whole blood (SWB) is blood that is more than 8 hours old and contains RBCs, plasma proteins, and small amounts of platelets and coagulation factors.2,5,6,13 SWB can be used for anemia with hypoproteinemia as well as for intravascular volume expansion and oxygen-carrying support.SWB should be kept for 28 to 35 days only, depending on the anticoagulant used, at 33.8°F to 42.8°F (1°C to 6°C).
Packed Red Blood Cells
pRBCs are harvested from 1 U of whole blood when it is separated into RBCs and plasma by centrifuging it and using an extractor. pRBCs contain concentrated RBCs (PCV is approximately 80%) and are the component of choice for increasing RBC mass in patients requiring oxygen-carrying support, such as those with anemia or bone marrow disorders. The shelf life of pRBCs is 28 to 35 days, depending on the anticoagulant used and how adequately the product is refrigerated. To prepare pRBCs for delivery, the component may be diluted with 0.9% sodium chloride (an isotonic solution containing no calcium) at up to a 1:1 ratio to reduce viscosity and improve flow during the transfusion. A calcium-containing solution should not be used to dilute pRBCs because it may cause lysis of the RBCs and activate clotting systems. Lactated Ringer’s solution, Normosol-R (Abbott Laboratories, Abbott Park, IL), 5% dextrose in water, and hypotonic sodium chloride also should not be used to dilute pRBCs for transfusion. These solutions should not be used because they cause RBC clumping, swelling, and hemolysis by diffusing into the RBCs.
Plasma
FFP is harvested from 1 U of whole blood and contains coagulation factors and plasma proteins. Indications for this product are coagulation deficiencies, anticoagulant rodenticide toxicity, liver disease, disseminated intravascular coagulation, and acute hypoproteinemia. FFP is stored at -4°F to -22°F (-20°C to -30°C) for up to 1 year to preserve its coagulation factor. After 1 year, FFP becomes known as long-term storage plasma and can be stored for an additional 4 years. It contains plasma proteins, minimal platelets, and active coagulation factors, such as stable vitamin K-dependent factors II, VII, IX, X, fibrinogen, and antithrombin III. Long-term storage plasma is indicated for hypoproteinemia.
Plasma should be thawed properly; if it does not reach 98.6°F (37°C), the hemostatic proteins will not fully dissolve; therefore, they will be less available to the patient.5 On the other hand, hemolysis and protein denaturation may occur if the plasma reaches a temperature greater than 98.6°F (37°C).5 It is important to remember that plasma is fragile when frozen and the bag may crack or break if it is manipulated too frequently before it is completely thawed. Plasma should be thawed by placing the bag into a warm-water bath that does not exceed 98.6°F (37°C) to allow thawing. Plasma takes about 30 minutes to an hour to thaw. Never use a microwave to thaw plasma because it is hard to regulate the temperature and overheating will occur. To guard against the effects of freezer malfunction, a rubber band may be placed around the frozen bag of plasma before it is put in the stock freezer. If the plasma thaws and then refreezes, the rubber band will move and the indentation will be different.
Platelet-Rich Plasma and Platelet Concentrate
PRP and platelet concentrate are harvested by centrifuging FWB at a rate slower than that used for production of pRBCs and plasma.4 Because refrigeration causes platelet dysfunction, FWB should be centrifuged at room temperature to preserve platelet function and viability.5 Once centrifuged, the plasma is expressed with an extractor until the RBC layer is entered. PRP contains platelets, coagulation factors, and plasma proteins. It is used to stop severe, uncontrolled, or life-threatening bleeding in patients with decreased platelets or platelet function but not in those with increased consumption or destruction of platelets. PRP is difficult to store and has a short life span but can be used within 48 hours if kept at room temperature and protected from light. If the product is not available for immediate administration, FWB should be used instead.
If platelet concentrate is needed, a collection bag with two satellite bags is used. PRP is further centrifuged into one satellite bag, and all but 50 ml of the plasma is expressed into the second satellite bag. The remaining product is platelet concentrate.
Cryoprecipitate
Cryoprecipitate is prepared from 1 U of FFP by using a triple-bag collection system. Cryoprecipitate is the cold, insoluble portion of plasma that precipitates after FFP has been thawed slowly in the refrigerator at 33.8°F to 42.8°F (1°C to 6°C) for about 12 to 18 hours.The precipitate forms when approximately 90% of the FFP has thawed and is a slushy consistency. The slushy FFP is centrifuged, and the plasma is expressed into the third satellite bag, leaving behind a white, foamy precipitate that sticks to the sides of the second satellite bag. About 10 to 15 ml of plasma should be left in the bag to mix the cryoprecipitate at the time of administration. The cryoprecipitate is then stored at -4°F to -22°F (-20°C to -30°C) up to 1 year after the FFP collection date. Cryoprecipitate contains von Willebrand factor, fibrinogen, and factor VIII and is used to treat von Willebrand’s disease, hemophilia A, and fibrinogen deficiency.2,4,5,12 The clear fluid on top of the cryoprecipitate is called cryosupernatant and can be used to treat animals with hemophilia B (factor IX deficiency).
Administration of Blood Products
Several routes may be used for administering blood products. With the intravenous route, which is the most common and most effective, the infused RBCs and plasma are available to the general circulation immediately. The intraosseous route is ideal only when vascular access is difficult or unsuccessful and is most commonly used in neonates. Common sites for intraosseous transfusion are the trochanteric fossa of the femur, the wing of the ilium, and the shaft of the humerus. With this route, the infused cells and proteins are available to the general circulation within minutes of delivery, but there is a risk of osteomyelitis. The intraperitoneal route is painful and should not be used unless absolutely necessary. With this route, the infused RBCs are completely absorbed, but the absorption is delayed. At 24 hours, only about 50% of the infused RBCs and proteins will have reached the general circulation; at 28 to 72 hours, 70% will have become absorbed. In addition, the intraperitoneal route carries a risk of peritonitis.
A blood administration set with a micropore filter (180 to 220 µm) should always be used when preparing blood products for transfusion to prevent debris and blood clots from passing to the patient.5,14 Although warming is not required unless the product is frozen, it may be a good idea to bring the transfusion recipient’s body temperature up to normal or prevent the temperature from dropping further if the patient is hypothermic or at risk for hypothermia. The temperature of blood products should never exceed 98.6°F (37°C); blood is a great growth medium for bacteria, and increased warmth induces bacterial growth.An alternative to warming a blood product is to run the administration set through a warm-water bath during transfusion. The recipient should never be disconnected from the equipment during the transfusion because of the potential for introduction of bacteria.
Monitoring
Before the transfusion, baseline evaluations of the recipient’s attitude, rectal temperature, pulse rate and quality, respiratory rate and character, mucous membrane color, and capillary refill time are made. These measurements are compared with those obtained during the transfusion process. After the baseline study, the transfusion is started slowly (one of the most common causes of transfusion reactions is starting the transfusion of whole blood or component at too high of a rate) and the patient is monitored for acute transfusion reaction.
The patient is monitored continuously for any signs of reaction, and the evaluations made at baseline are reassessed every hour until the transfusion is complete. If there is any sign of reaction at any time during the transfusion, the transfusion should be discontinued immediately and a doctor notified. The decision whether to continue the transfusion usually depends on the severity of the reaction. The veterinarian may order saline, diphenhydramine, and steroids to treat shock and stabilize cell membranes. Oxygen should be given and treatment for disseminated intravascular coagulation started if necessary. Transfusions should be completed within 4 hours to reduce the risk of bacterial contamination.
Each veterinary practice should have its own protocol for monitoring transfusions so they are done the same way every time. If a written protocol is provided, the center’s staff can detect transfusion reactions at their onset so that appropriate action can be taken.
Transfusion Reactions
Reactions that occur during or after a transfusion fall into two categories: immune-mediated and non-immune-mediated reactions. Immune-mediated reactions are further classified as hemolytic or nonhemolytic. Hemolytic reactions can be acute or delayed.
Immune-Mediated Reactions
Acute transfusion reactions are the result of preexisting antibodies (e.g., a reaction caused by a transfusion of feline type A blood to a cat with type B blood) or sensitization from a previous transfusion (e.g., a reaction in a previously sensitized DEA 1.1-negative dog.). Although acute transfusion reactions are the rarest type of reaction, they are also the most serious. The earliest clinical sign is hyperthermia, which is why body temperature monitoring is so important. Another early sign of an acute reaction is vomiting; other signs include tachycardia, tachypnea, weakness, muscle tremors, facial swelling, agitation, vocalizing, hypotension, hemoglobinemia, and hemoglobinuria.2,5,9,16
Delayed transfusion reactions can occur 2 to 21 days posttransfusion and are the most common reactions after transfusion. The hallmarks of a delayed reaction are a shortened survival of transfused RBCs and a falling PCV.
Nonhemolytic reactions may be the result of antibodies to RBCs, leukocytes, platelets, or plasma proteins and are most often transient. Clinical signs of these reactions are anaphylaxis, urticaria, pruritus, hyperthermia, tachypnea, dyspnea, vomiting, and neurologic signs.
Non-Immune-Mediated Reactions
Non-immune-mediated reactions have several causes. Asymptomatic hemolysis caused by trauma to RBCs occurs when blood products are overheated, leading to protein denaturation and a potential increase in bacterial growth during transfusion. Delivering an RBC product with a PCV greater than 80% may also cause problems during transfusion. Asymptomatic hemolysis may also occur when transfusing an RBC product that was frozen, warmed, and then placed back in the refrigerator. RBC trauma can also be caused by the use of catheters or needles that are too small for collecting or administering blood products.
Non-immune-mediated reactions may result from bacterial pyrogens or sepsis caused by contamination of blood products that have been improperly collected, stored, or administered. If the plasma supernatant of a blood product is dark brown to black, the product should not be used because this coloration indicates digested hemoglobin from bacterial growth. If such a contaminated product is administered, fever may develop within 15 to 20 minutes into the transfusion but usually subsides within 2 to 4 hours after completion of the transfusion.
Another non-immune-mediated reaction is citrate toxicosis, which is the result of a disproportionate blood:citrate ratio. Citrate toxicosis often occurs in patients receiving a massive transfusion, especially patients with liver disease. It may also result when not enough blood is drawn into a collection bag containing citrate anticoagulant at the donation stage. For this reason, this type of bag should not be used if at least 350 to 400 ml of blood cannot be drawn from the donor. Clinical signs of citrate toxicosis include involuntary muscle tremors, cardiac arrhythmias, and decreased cardiac output.Animals with liver disease should be transfused only with fresh blood products to avoid ammonia buildup (e.g., recently collected pRBCs should be used instead of pRBCs that will expire in 2 days).
Because blood is a colloid, volume overload may be another concern in transfusion patients. Volume overload can be prevented by delivering only the type and amount of the component necessary to treat the specific disorder. If volume overload is a concern, the patient should be observed frequently with lung auscultation and central venous pressure monitoring. Signs of volume overload are coughing, dyspnea, cyanosis, tachycardia, and vomiting.
FAQ
Why transfuse?
There may be various situations when a pet might need a transfusion, depending on the underlying cause or disease process. A common scenario would be haemorrhage (blood loss). For example externally and obviously through a road traffic accident. Or internally (and usually less obviously), with either a tumour that is bleeding into a body cavity, or potentially rodenticide (warfarin-rat poison) toxicity.
Other causes of anaemia which may necessitate a blood transfusion, include immune mediated haemolytic anaemia (where the body’s own immune system inappropriately attacks and destroys its own red blood cells), or a bone marrow disease, where there is inadequate production and replenishment of red blood cells.
How often do dogs and cats need a transfusion?
In haemorrhagic or haemolytic diseases the bone marrow typically remains healthy and within 3-5 days. Tthe body starts to show signs of new and increased red blood cell production itself (regenerative anaemias). With these conditions, a blood transfusion(s) would help stabilise the patient by improving the oxygen carrying capacity, until an adequate level of spontaneous regeneration has occurred. Additionally, with haemolytic diseases, a blood transfusion may “buy some time” until other medications can start to effectively control the underlying disease and stop the red cell destruction.
In contrast, with the majority of bone marrow disease, adequate regeneration by the patient may never occur (the anaemia is therefore described as non-regenerative). In such cases, sadly, a blood transfusion would only be expected to offer a palliative, supportive and short-term benefit.
What does blood do?
Blood is vitally important in maintaining a “balance” within the body (homeostasis) and has a number of functions. Chiefly, it carries oxygen and nutrients around the body and lungs for tissue metabolism, whilst also removing carbon dioxide and waste products. Alongside this, it carries cells of the immune system which fight infection and transports hormones.
What are the signs of anaemia?
A lack of adequate circulating blood volume, red cells or haemoglobin is called anaemia. This results in symptoms that include weakness, lethargy, pallor (pale mucous membranes), and increased heart and respiratory rates. Additionally, your vet may pick up a heart murmur, fever, jaundice and enlargement of the liver and or spleen. Pica (eating of substances of no nutritional value such as dirt or cat litter), is not infrequently seen in cats with anaemia and can be a relevant part of the history.
What dictates when a blood transfusion is needed?
The need for a blood transfusion will depend upon numerous factors. It, of course, varies on a case by case basis. Your vet would discuss these with you, as an owner of an anaemic pet.
Importantly this will include the speed at which the anaemia has developed. If very rapid, the body will have had an inadequate amount of time to respond and compensate and the animal is bound to be struggling.
Furthermore, the severity of the anaemia is a factor; clearly the more anaemic an animal is, the more severe the associated clinical signs.
Cats differ from dogs though. Given their relatively short red blood cell lifespan (70 days in cats compared to 120 days in dogs) and relatively small blood volume. They are unfortunately more prone to developing anaemia. Like many of the diseases we see in cats however, the anaemia may have actually been developing over a number of weeks and is tolerated well initially due to cat’s activity levels and haemoglobin structural alterations. Symptoms may appear suddenly and dramatically when they hit a “crisis” point or level however.
Do animals have blood types like humans?
Blood types do exist in dogs and cats albeit with some differences to humans. It is known that the presence of certain proteins or sugars on the red blood cell membrane determine the exact blood group of any animal and that these differ between individuals.
In dogs the DEA (dog erythrocyte antigen) system documents more than 12 different blood types. The DEA 1.1 group (positive or negative) is the most important (and only usually screened for) type. A universal donor dog would have blood type DEA 1.1 negative. Such dogs can safely donate blood to any other dog on a first occasion. Virtually no risk exists in this situation since dogs do not possess naturally occurring antibodies (against other blood group types). Such antibodies do however form a few days after a first transfusion, so second and subsequent donations must be both typed and cross-matched.
The complete opposite is true in cats. Their blood group system is the AB system and cats DO possess naturally occurring, strong antibodies against other blood group types. Both the donor and recipient cat must therefore be typed ahead of any planned transfusion, otherwise fatal reactions may occur.
In both cats and dogs, certain breeds are prone to belong to particular blood group types. For example, greyhounds are often DEA 1.1 negative and most domestic short hair cats in the UK would be blood type A.
Do cats and dogs have blood types?
Yes! Dogs and cats have specific blood types.
The dog typing system is called DEA, which stands for Dog Erythrocyte Antigen. Each DEA number represents a different erythrocyte (red blood cell) antigen (protein on the surface of the cell). The six DEAs tested for when blood typing are 1.1, 1.2, 3, 4, 5, and 7. A dog can be positive or negative for any of these antigens. They don’t have pre-existing antibodies to the antigens, but once a dog has received a transfusion, it will develop antibodies to any antigens it did not have originally, and could have a reaction if it is exposed to those antigens a second time. For this reason, we want to give a compatible donation. Almost every dog has DEA 4, so a dog that ONLY has DEA 4 is considered a “universal” donor and can donate to a dog with any blood type.
The cat typing system is simply A, B or AB although a new antigen called Mik has more recently been identified. Unlike dogs, cats possess strong naturally occurring antibodies to the opposite blood type. This means that while most dogs could tolerate a first transfusion from any other dog (before they develop antibodies to a type that isn’t theirs) without serious consequences, cats can not. A few drops of A blood given to a B cat can lead to fatal consequences in short order, so it is crucial that both the donor and the receiver of the blood have the same blood type.
Several kits are now available for testing for blood type, but it is still time consuming when minutes may count in a critical patient.
For that reason, if we suspect a patient may require a transfusion, we will do typing and “matching” ahead of time so that we can be as ready as possible should the need arise for a transfusion.
As transfusion medicine continues to advance, it is important for technicians to be aware of the latest information so they can keep up with this ever-changing field. Transfusion medicine is sparking the interest of more and more technicians, and they are taking the initiative to educate themselves about it. As technicians become more knowledgeable in this area, an increasing number of blood donor programs are being set up in private practices. It is rewarding to see animals donate blood to help save lives, even though they do not understand what is happening to them. All they know is they get a cookie when it is over. As long as veterinary blood donor programs continue, blood products will be available and lives will be saved every day.
![]()

Blood transfusion in veterinary medicine
Compiled & Shared by- Team, LITD (Livestock Institute of Training & Development)
Image-Courtesy-Google
Reference-On Request.